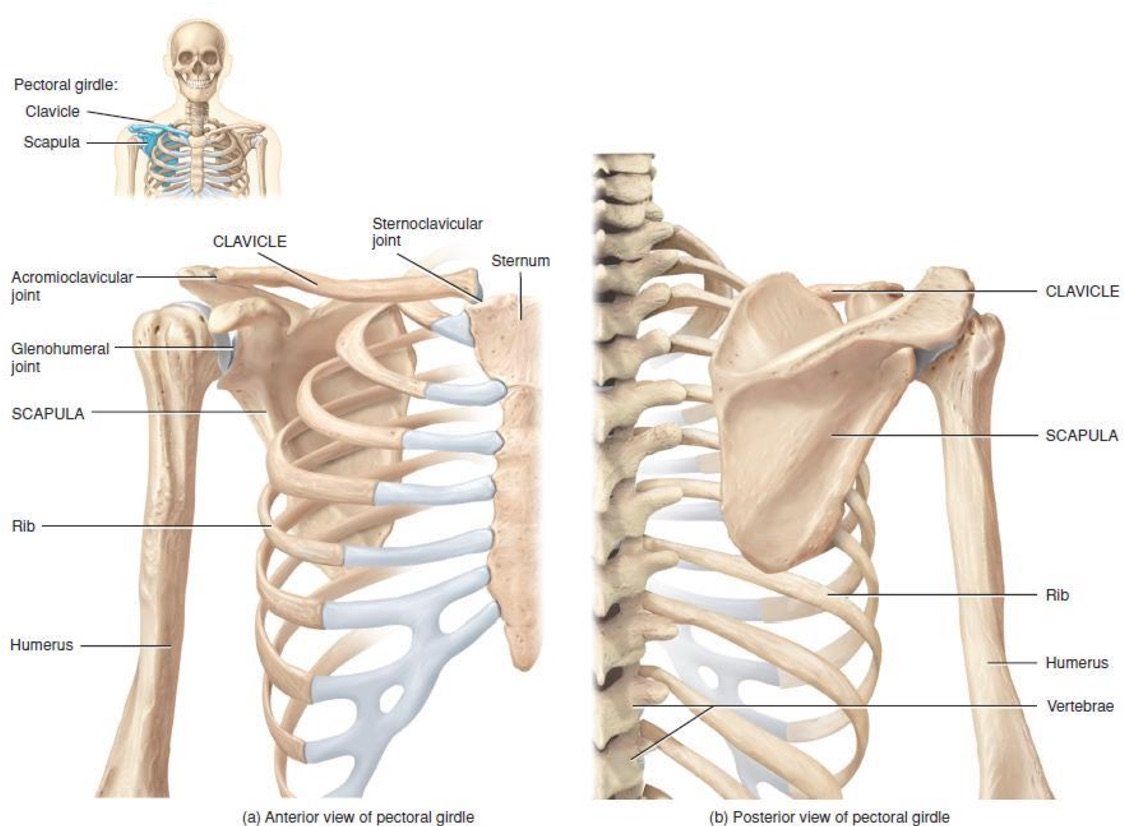
Functional Health of the Shoulder Girdle
Common issues affecting the shoulder complex
Below are some functional syndromes that may lead to chronic pain or injury. Poor posture is often caused by lifestyle factors. These syndromes can help explain chronic pain and injuries incurred during activities.
Upper crossed syndrome - the complex relationship between short-tight muscles and long-weak muscles, which support posture and movement connected with the shoulder girdle, thoracic spine, cervical spine and thoracic cage. The result can lead to a cross pattern of overactive muscles with countercross underactive muscles.
Upper crossed syndrome observable traits:
- Head forward
- Shoulders forward and elevated
- Hunched back
- Arms hang in front of body
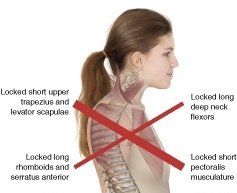
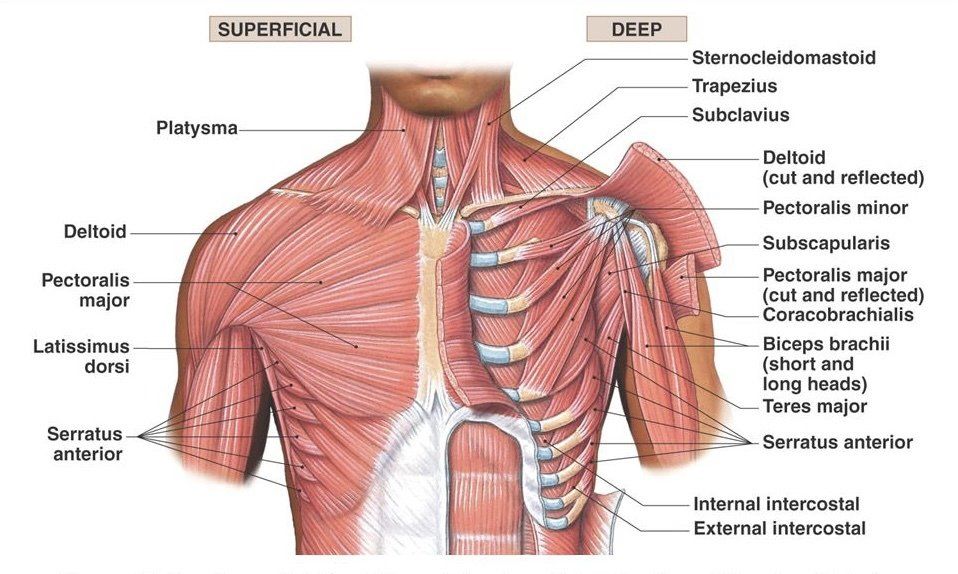
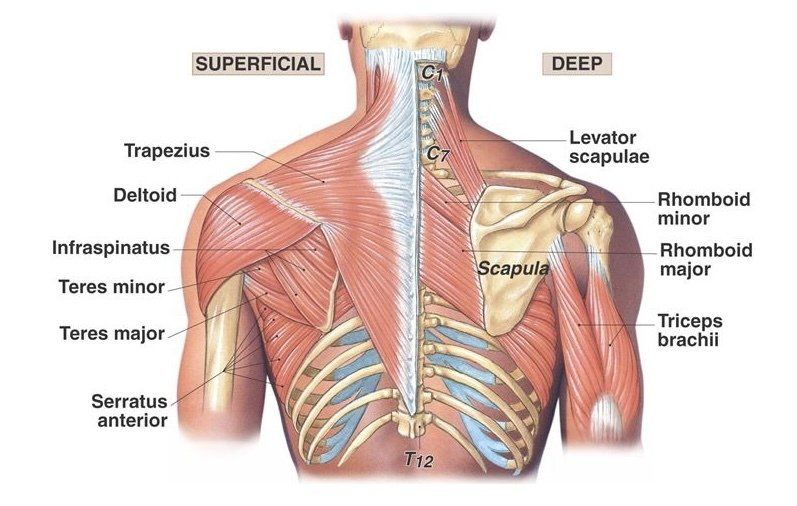
An example may be tight pectoral muscles and weakened rhomboids and mid trapezium. The rhomboids and mid trapezium may become over active and ache when counter balancing the postural deviance cause by tight pectoral muscles. This condition is often exacerbated through prolong periods of sitting over a desk or work station.
Kyphosis - Kyphosis is a postural syndrome of the upper back. The shoulders appear rounded and the upper back is hunched. There are postural similarities to upper crossed syndrome. Whilst upper crossed syndrome may explain the muscular imbalance, kyphosis describes the skeletal deformity.
Scapulothoracic stabilisation - the shoulder complex relies on the scapular stabilisers to maintain scapular position throughout movement of the shoulder girdle. Scapular dyskinesis can decrease function of the shoulder complex and increase the risk of injury.
Muscles involved are:
- pectoral minor, rhomboids, trapezius, lavator scapulae, sarratus anterior
Scapulohumeral rhythm - describes timing of movement at glenohumeral (ball & socket joint of the shoulder) joint and scapulothoracic joint during shoulder elevation. At full elevation the humeral elevation to scapulothoracic upward rotation ratio is 2:1. This is a nonlinear ratio during shoulder movement through different planes. Scapulohumeral rhythm serves two purposes:
- improves range of motion of the shoulder girdle
- prevents shoulder impingement (subacromial impingement)
Glenohumeral stability (shoulder Joint)
Glenohumeral stability depends on a combination of capsuloligamentary stabilisers (static stabilisers) and musculotendinous stabilisers (dynamic stabilisers).
Musculotendinous stabilisers assist in holding the humerus head in the glenoid fossa (shoulder ball and socket joint) during movement.
- Primary dynamic stabilisers are - rotator cuff muscles (supraspinatus, infraspinatus, teres minor, subscapularis), deltoids.
- secondary dynamic stabilisers are - terres major, latissimus dorsi, pectoral major.
As far as function is concerned, skeletal muscles are predominantly involved in posture and in movement. These muscles are engaged in stabilising and controlling the motion of the shoulder complex.
Weak muscles are invariably inhibited by the dominance of tight muscles. This can then lead to instability and poor movement patterns of the shoulder complex. Chronic neck and back pain as well as acute shoulder injury can arise as a result of poor movement patterns and shoulder instability.
Acute shoulder injuries or chronic conditions may be exacerbated by postural and mobility syndromes. Some sports, activities and lifestyle constraints can contribute to shoulder complex injuries and chronic pain. Chronic conditions in the shoulder complex can include pain and dysfunction in the upper back, neck and chest.
Common condition related to the shoulder complex:
- subacromial impingement - injury to tendons or bursar
- thoracic and cervical outlet syndrome - reduced muscle strength or tingling down the arms and fingers
- SLAP lesions - tears and impingement
- rotator cuff strain and tears - weak movement pattern and pain
- dislocation - torn ligaments, surgery
- frozen shoulder - restricted elevation of arms above the head
- periscapular pain - upper back and neck tension, stress and pain.
In most instances relief, improvement or correction can be achieved through rehabilitation exercise and therapy. Primarily, tight and short muscles should be corrected before strengthening weak muscles. However, improving muscle tonicity may help tissue elasticity.
In a sporting context poor functional movement patterns (dyskinesia) can lead to overuse injuries. The sports massage therapist will test, assess and treat most musculoskeletal conditions related to the shoulder complex. This will include spinal, upper and lower limb condition that can influence the functional motion of the shoulder girdle.
The sports massage studio offers treatment plan for athletes, exercise enthusiasts and occupational conditions.
